Nursing progress notes are an integral part of a patient’s medical record, documenting the ongoing care and treatment provided by nurses and other medical practitioners. These notes provide an accurate and complete picture of a patient’s current health status, including any new or worsening symptoms, vital signs changes, and treatment responses. By keeping detailed and up-to-date nursing progress notes, healthcare professionals can enhance communication between team members, track patient outcomes, and make informed decisions about ongoing care. Furthermore, using a template to create nursing progress notes can help ensure that all relevant information is accounted for and that notes are consistently structured and easy to read, ultimately leading to better patient care.
What Are Nursing Progress Notes?
A nursing progress note is a crucial component of a patient’s medical record that documents the ongoing care and progress of a patient during their hospital stay or healthcare treatment. These notes are typically written by nurses and serve as a means of communication among healthcare professionals involved in a patient’s care. Nursing progress notes provide a concise summary of the patient’s condition, treatment interventions, response to treatment, and any notable changes or updates in their health status. These notes serve as a chronological record of the nursing care provided, including assessments, vital signs, medications administered, procedures performed, patient education, and any significant observations. Nursing progress notes are essential for ensuring continuity of care, facilitating effective communication, and providing a comprehensive picture of a patient’s healthcare journey.
What’s the Difference Between Nursing Progress Notes and SOAP Notes?
Nursing progress notes and SOAP (Subjective, Objective, Assessment, Plan) notes are both commonly used documentation formats in healthcare, but they differ in their focus and purpose. Nursing progress notes primarily capture the nursing care provided and the patient’s response to that care. They focus on the patient’s physical, emotional, and psychological well-being, including assessments, interventions, and observations related to nursing care. Nursing progress notes also document important conversations with the patient and their family, highlighting patient preferences, concerns, and goals.
On the other hand, SOAP notes are a structured format used by healthcare professionals, including physicians, to document patient encounters and medical assessments. SOAP notes consist of four sections: Subjective (patient’s description of symptoms), Objective (observable data and measurements), Assessment (diagnosis or impression), and Plan (treatment plan). While nursing progress notes may include subjective and objective information, their primary focus is on the nursing care provided and the patient’s response to that care, rather than making a formal medical diagnosis or outlining specific treatment plans. Nursing progress notes and SOAP notes complement each other, providing a comprehensive view of a patient’s care from both nursing and medical perspectives.
Fun Fact: A nursing progress note is essential for patient care and medical team members, but it can also help lawyers in court. Keeping accurate, detailed information is crucial to help your patients, but it can also be used as evidence in court if any disputes or issues arise later.
How Can a Nursing Progress Note Example Help You?
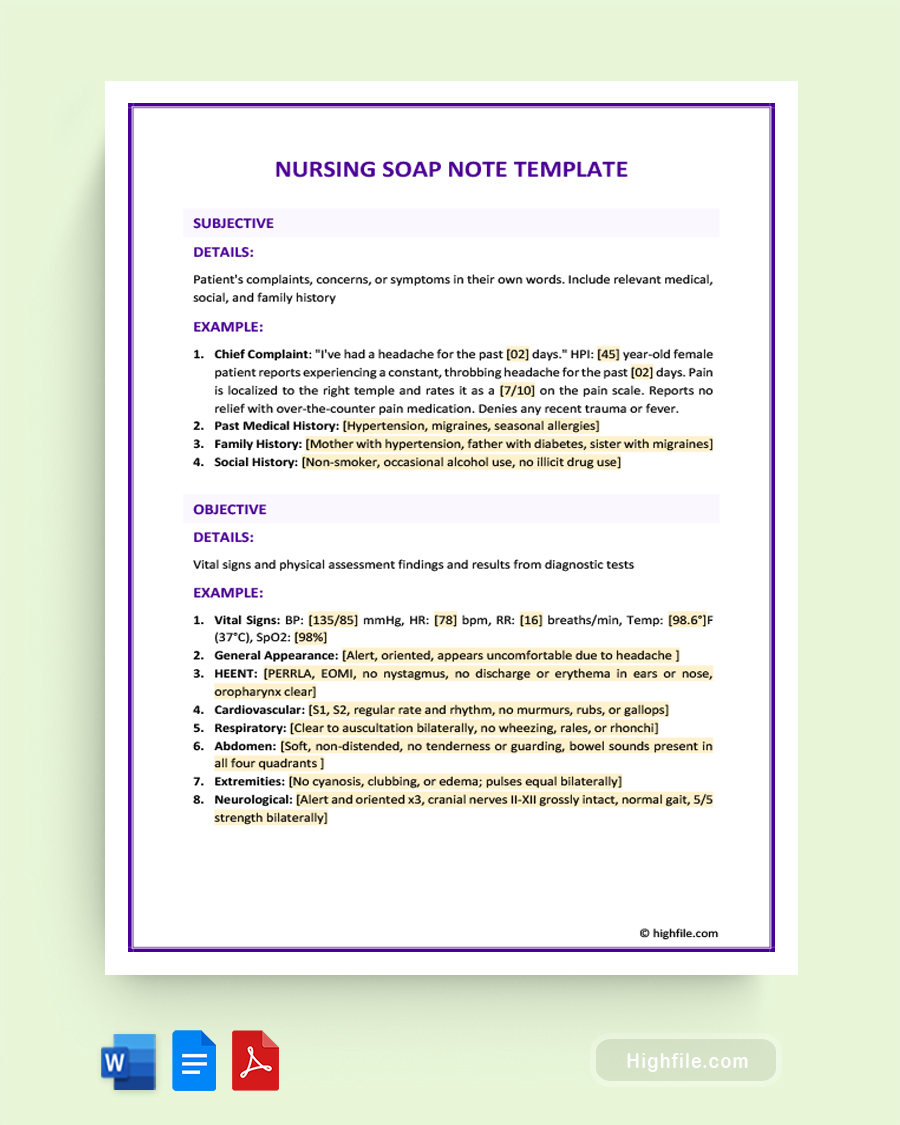
A nursing progress note example can be an invaluable resource for nurses and healthcare professionals, especially those new to the field or seeking to improve their documentation skills. By examining a well-crafted nursing progress note example, nurses can gain insights into the proper structure, content, and language used in these notes. They can learn how to effectively summarize patient assessments, interventions, and observations, ensuring that the notes accurately reflect the care provided. Additionally, a nursing progress note example can demonstrate the importance of including relevant and concise information and avoiding jargon or abbreviations that may hinder comprehension.
Furthermore, reviewing nursing progress note examples can enhance communication and collaboration among healthcare professionals. It allows nurses to understand the information their colleagues have documented, facilitating continuity of care and ensuring that all relevant details are considered. By adhering to best practices demonstrated in nursing progress note examples, healthcare professionals can maintain accurate and comprehensive documentation, which is essential for patient safety, quality of care, and legal purposes.
Important Note: Efficient, consistent communication is crucial in healthcare. As a result, using a template or other standardized blueprint for creating Nursing Progress Notes is vital. No matter how many people read or contribute to these notes, having a simple consistent format makes it easier for everyone on the team to communicate patient information quickly and easily, which can help you provide optimal care.
Essential Elements of A Nursing Progress Note
A good nursing progress note should be straightforward and accessible for all team members to understand. Below are the essential elements to include.
- Patient Information: Include their name, age, gender, admission date, and room number.
- Vital Signs Table: This should list the date and time, temperature, blood pressure, respiratory rate, and heart rate.
- Assessment Table: This chart should have space for date and time, assessment, findings, and interventions.
- Plan of Care Chart: Include the date and time, goals, interventions, and evaluation.
How to Compose a Nursing Progress Note
Nursing progress notes are a vital record of the care provided to patients, documenting their ongoing health status, any changes in their symptoms, and responses to treatment. Accurate and timely progress notes can help healthcare professionals make informed decisions about further care and treatment. To compose effective nursing progress notes, it’s essential to keep the following tips in mind:
- Identify the nurse and patient.
- Include the date and time of the note.
- Use concise and specific language.
- Document new or changing symptoms or concerns.
- Record vital signs and other objective measures.
- Note the patient’s response to treatments or interventions.
- Include any follow-up actions or plans.
- Sign and date the note to ensure accuracy and accountability.
Pro Tip: One of the most crucial aspects of a Nursing Progress note is the changes to the patient and their response to treatment. Be sure to include these as identifying them in a timely manner can significantly impact patient care. Your note will be used to help team members coordinate and communicate, so a well-composed note can increase positive outcomes for the patient and communicate vital details.
Key Points
Nurses and other medical practitioners use nursing progress notes to document patient care and track their progress throughout the healthcare journey. These notes serve as a means of communication among healthcare professionals, ensuring the continuity of care and facilitating effective collaboration. By documenting assessments, interventions, and observations in nursing progress notes, nurses can provide an accurate and comprehensive picture of a patient’s condition and response to treatment. This helps healthcare professionals make informed decisions, tailor care plans, and monitor the effectiveness of interventions. Moreover, nursing progress notes support legal and regulatory compliance, quality improvement efforts, and reimbursement processes. Using a template to create nursing progress notes further enhances efficiency and consistency in documentation, ensuring that all essential information is included and reducing the risk of errors or omissions. Templates provide a standardized framework, guiding nurses in organizing and presenting information in a structured and systematic manner, ultimately contributing to improved patient care and communication among healthcare teams.